![Signals From [Space]](https://substackcdn.com/image/fetch/w_80,h_80,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F55686857-6b99-45a6-ac0f-09c9f023f2a0_500x500.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/e_trim:10:white/e_trim:10:transparent/h_72,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F4d588ac1-7fac-4bd4-829d-fc7b4e8f1326_1512x288.png)
![Signals From [Space]](https://substackcdn.com/image/fetch/w_36,h_36,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2F55686857-6b99-45a6-ac0f-09c9f023f2a0_500x500.png)



In today’s show we hear from Dr. Yasir Qazi, a clinical associate professor of medicine and medical director of the kidney pancreas transplant program. He shares his journey into nephrology and transplantation, and discusses the evolution of kidney transplant, the importance of pancreas programs, and the complexities of the organ donation process— including the role of OPO and UNOS. Dr. Qazi highlights the challenges of kidney discard rates, racial disparities in transplant wait times, and the need for better patient education and financial incentives to increase organ donation. He also shares personal stories that illustrate the emotional toll of his work and the impact of organ donation on patients' lives.
Guest Bio
After serving as an assistant professor of medicine at Erie County Medical Center at the State University of New York in Buffalo, Dr. Qazi came to southern California to head the Kidney-Pancreas Transplant Program at Keck School of Medicine at USC. Dr. Qazi has received nearly $2 million in research grants and has several other studies recently submitted for approval. While in Buffalo, Dr. Qazi was invited to lecture on pancreas transplantation at a number of area medical centers and continues to author numerous peer reviewed articles and abstracts for medical journals. Educated in India, Dr. Qazi was consistently one of the academic leaders among his medical school classmates and he continues to demonstrate his talents and devotion to medicine as an educator, researcher and practitioner. Find Dr. Qazi’s awards and publications here.
This edition of Signals was made free for all readers thanks to Roivios, the team developing the world’s first renal assist device. Check out JuxtaFlow, a clinical-stage solution for renal insufficiency. Thanks team!
Keywords
nephrology, transplantation, kidney transplant, pancreas transplant, organ donation, KDPI, LYFT, racial disparities, transplant wait times, healthcare equity, patient education
In this episode, we cover:
00:50 Dr. Yasir Qazi’s Journey
02:53 The Evolution of Nephrology and Transplantation
05:59 Understanding the Kidney Transplant Process
08:33 The KDPI Scoring System Explained
11:24 Challenges in Organ Donation and Discard Rates
14:26 Racial Disparities in Kidney Transplant Wait Times
17:10 Strategies for Increasing Access to Transplantation
39:12 The Urgency of Transplantation
41:13 Financial Incentives in Organ Donation
45:39 Innovative Approaches to Increase Donor Awareness
48:13 Disparities in Transplant Outcomes
51:02 The Emotional Weight of Organ Donation
53:41 The Importance of Teamwork in Transplantation
Takeaways
Mentorship and Inspiration Shape Careers: Dr. Qazi’s journey into nephrology and transplantation was influenced by mentors like Dr. Eli Friedman, whose expertise and guidance inspired him to pursue advanced training and leadership in the field. He highlights the value of strong mentorship in shaping a career in transplant medicine.
Why Start a Pancreas Program? Adding pancreas transplantation to his expertise was a deliberate effort to expand life-saving treatment options. Dr. Qazi’s determination to address unmet needs in transplantation led to milestones like establishing a pancreas transplant program in Orange County.
The Emotional Challenges of Organ Allocation Decisions: One of the hardest parts of Dr. Qazi's job is making critical decisions about accepting or declining organ offers. These choices are emotionally taxing because declining an organ might mean it goes unused, while accepting a less-than-ideal kidney carries risks for the patient. Balancing these factors impacts both patient lives and the efficient use of donated organs.
The Importance of Kidney Utilization and Education: With thousands of viable kidneys discarded each year, Dr. Qazi emphasizes the need to maximize organ usage and educate patients about their options. He also highlights how transplant centers are scrutinized for their acceptance rates, reflecting a broader shift toward accountability and access.
Understanding KDPI and EPTS Scores for Better Matching: Dr. Qazi explains the importance of the Kidney Donor Profile Index (KDPI) and the Estimated Post-Transplant Survival (EPTS) scores in organ allocation. KDPI assesses the quality of the donor kidney, while EPTS estimates the recipient's expected longevity post-transplant. Utilizing these metrics helps match kidneys more effectively with recipients, optimizing transplant outcomes and longevity.
Addressing Disparities in Organ Allocation: Changes in kidney allocation systems, such as crediting time spent on dialysis before being waitlisted, have reduced racial disparities in access to transplantation. Dr. Qazi underscores the ongoing need to refine policies to ensure equity.
Living Donor Ethics and Support: While live kidney donation is life-saving, Dr. Qazi raises ethical concerns about incentivization models. He advocates for long-term health coverage for donors instead of financial incentives to ensure equitable participation without exploiting disadvantaged populations.
AI Could Enhance Decision-Making in Transplantation: Dr. Qazi is optimistic about the role of artificial intelligence in future transplant medicine. AI could assist in analyzing complex data to predict organ viability and patient outcomes more accurately. By incorporating AI into decision-making processes, transplant centers may reduce organ discard rates and better tailor matches between donors and recipients.
Transforming Lives Through Transplantation: Dr. Qazi reflects on the profound impact of organ donation, highlighting stories of hope and generosity that transcend divisions. He views transplantation as a testament to human connection and resilience.
References
Below you’ll find studies, reports, datasets & media mentioned during the show.
USRDS: The United States Renal Data System (USRDS) is a national data system that collects, analyzes, and distributes information about chronic kidney disease (CKD) and end-stage renal disease (ESRD) in the United States.
The SRTR Database. SRTR receives data collected by other organizations, manages and analyzes these data, and supplies data, summary reports, and analyses to the transplant community. The final SRTR database consists of many data tables with many components, including data on the transplant waiting lists, the donor/recipient matching process, deceased donors, living donors, and transplant recipients.
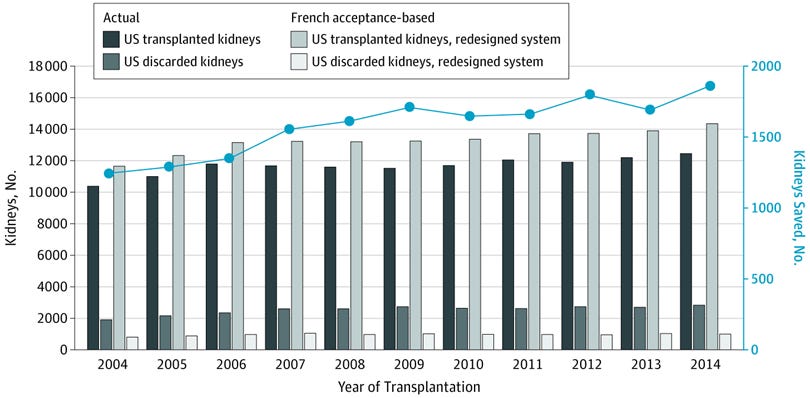
Study: Disparities in Acceptance of Deceased Donor Kidneys Between the United States and France and Estimated Effects of Increased US Acceptance. This study asks the critical question: would a more aggressive approach to organ acceptance provide a benefit to wait-listed kidney transplant candidates? Here’s what they found… (JAMA)
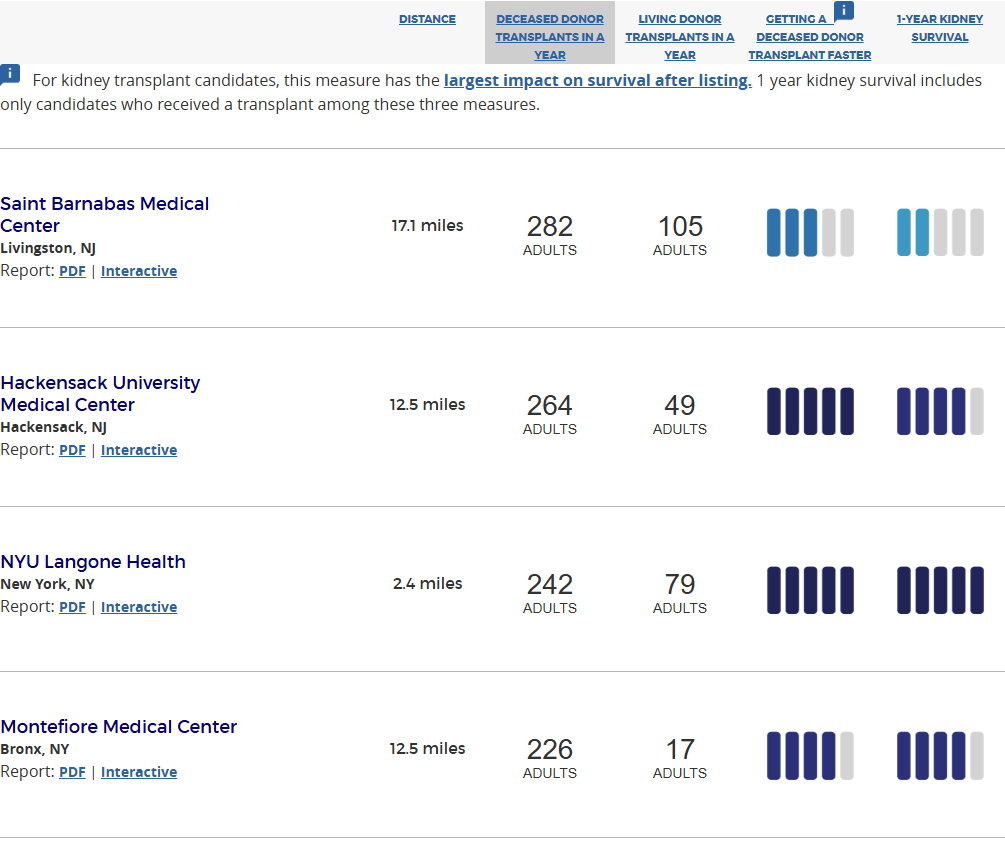
Transplant Coach: Find low-wait time hospitals and apply directly from Transplant Coach, reducing wait time by up to 75%.
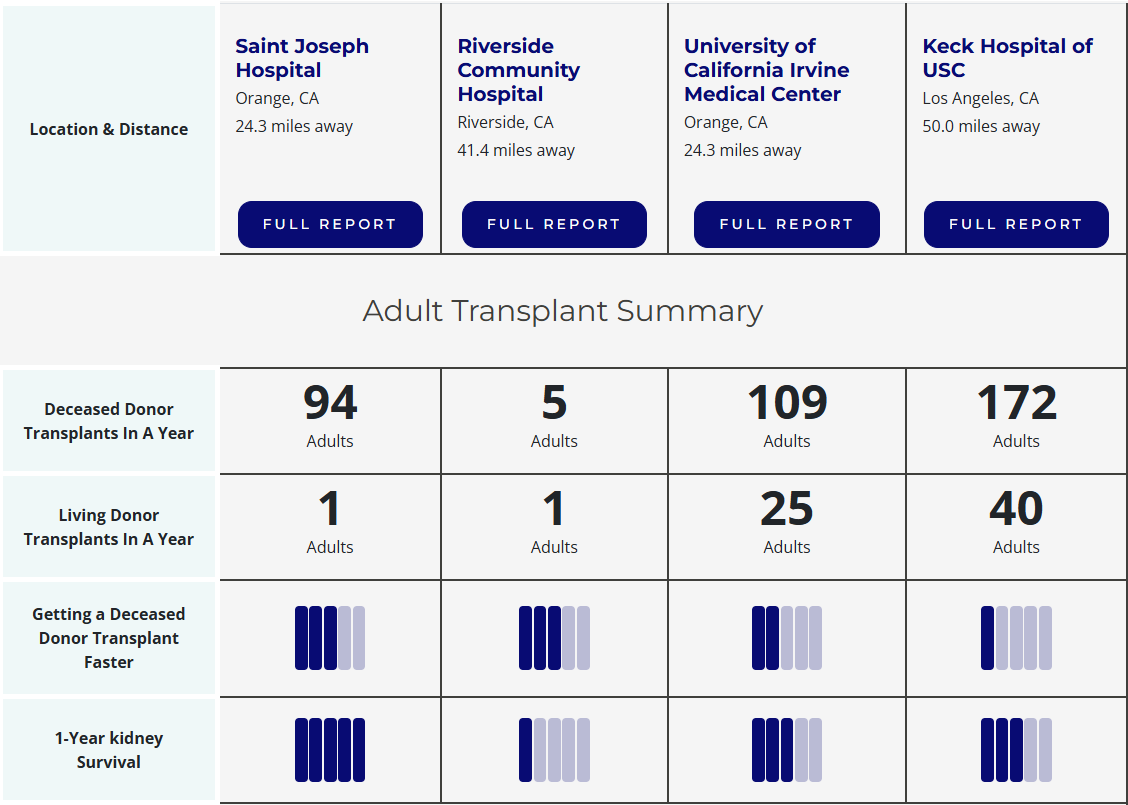
Kidney Transplant Decision Aid: This SRTR subsite was created with input from patients with kidney disease and the doctors who care for them. It is intended to be used during your visit with your doctor as you learn about kidney transplant. You can use this site to compare transplant programs in your area and across the country. We’ve provided an example below of programs near Orange County, CA. (SRTR)
The Big Donor Show: TV kidney donor show revealed as hoax to provoke debate on organ shortages. “It was decried as the show that would break the reality TV format's back. The makers of the [The Big Donor Show] promised a one-off programme in which a terminally ill woman would chose which of three contestants would receive her kidneys when she died. But last night the show was revealed to be a hoax…to raise awareness about organ donation in the Netherlands. "If the Big Donor Show had been real, it would indeed have been shocking but facts illustrate that the reality is far more so. In staging this programme our goal has been to promote a debate about this crisis in the Netherlands. We have succeeded in spades." (The Guardian, 2007)
Report: Addressing disparities in kidney transplantation. The health disparities that lead to higher incidence of kidney failure in communities of color also lead to barriers in accessing kidney transplants. Race, older age, less social support, lower income, more comorbidities, type of insurance coverage, and fewer transplant learning activities have been associated with a lower probability of kidney transplantation. These disparities in kidney transplantation have been demonstrated in the data. (AKF)
Study: Race, Age, and Kidney Transplant Waitlisting Among Patients Receiving Incident Dialysis in the United States. Patients with kidney failure from racial and ethnic minority groups and older patients have reduced access to the transplant waitlist relative to White and younger patients. Although racial disparities in the waitlisting group have declined after the 2014 kidney allocation system change, whether there is intersectionality of race and age in waitlisting access is unknown... (Kidney Medicine, 2023)
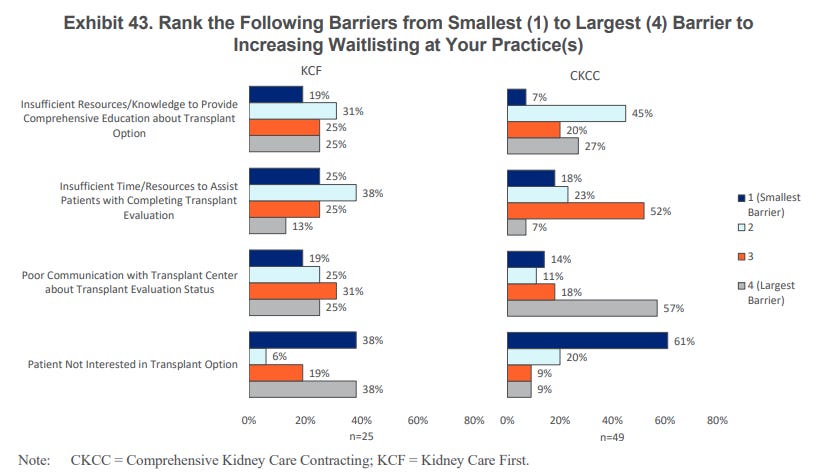
Report: Kidney Care Choices (KCC) Model PY 2022 Evaluation. The evaluation findings for the KCC Model’s first performance year (2022) provide insights
into the early effects of the model and lay the groundwork for future reports. More than half of KCF Practices reported poor communication with the transplant center (56%) and patient not interested (57%) as a large or the largest barrier to increased waitlisting, whereas insufficient time or resources to assist the patient with completing the evaluation process was reported as a small or the smallest barrier by 63% of KCF Practices… (CMS)
Banff Classification for Renal Allograft Pathology, 2022: Since its first consensus meeting in 1991, the Banff Classification Of Allograft Pathology has provided a framework for the reporting of renal allograft biopsies. It was the first classification system of its kind and answered the need for an international consensus on renal transplant biopsy reporting, providing guidance for clinical diagnosis and enabling meaningful comparison between research studies and clinical trials investigating the diagnosis, treatment and outcome in kidney transplantation. (Banff Foundation)
Leonard Cohen - “Who By Fire”
And who by fire? Who by water? Who in the sunshine? Who in the night time? Who by high ordeal? Who by common trial? Who in your merry merry month of May? Who by very slow decay? And who shall I say is calling?
Discussion
Here are a few top of mind questions. We’d love to hear from you in the Signals slack community and in the comments below.
What challenges have you seen or faced in establishing new transplant programs, particularly in underserved regions?
How can patient education and their voices play a bigger role in improving kidney utilization rates and shared decision-making?
What policy changes have you seen make a difference in improving access to transplantation? Where does IOTA fit in?
What’s your perspective on compensating kidney donors? Do you agree with Dr. Qazi’s idea that covering healthcare costs for donors is a better approach than financial incentives?
Have you seen examples where artificial intelligence improved organ allocation or reduced organ discard rates? What do you see as the biggest risks or limitations of relying on AI in these decisions?
Signals is made possible with the generous support of our sponsors. We are grateful to partner with organizations committed to advancing kidney care and innovation. Learn more about our sponsorships here.






Share this post